Pain Winter 2001
I. Introduction: pain is not just sensory experience. It has
survival value, but there are times when suppressing pain also has survival
value.
II. Primary afferents mediating pain are A delta (small myelinated)
and C (unmyelinated)fibers.
III. C fibers transmit the type of pain we will be studying.
A. Respond to stimuli that produce long lasting damage.
B. sensation produced is slow burning pain
C. C fiber endings are often polymodal nocioceptors
D. respond to chemicals released by damaged tissue.
1. histamine and prostaglandins and bradykinin are released
from damaged tissue. These can sensitize nociceptive nerve endings.
2. aspirin inhibits an enzyme used in the synthesis of
prostaglandins.
E. transmitter released by primary afferents are glutamate
and peptides. One of these peptides is substance P. But other peptides
may be involved in pain perception and substance P has additional functions.
1. glutamate responsible for fast synaptic responses,
peptides for slow.
2. capsaicin depletes endings of substance P. Therefore
it initially causes pain then causes insensitivity to pain.
3. central hyperalgesia due to windup that results from repetitive
input from C fibers. May be partially responsible for phantom limb pain.
Can avoid by anesthetizing spinal cord during amputation.
IV. opiate receptors
A. For a long time morphine was a drug in search of receptor.
Naloxone.
B. opiate receptors were discovered by looking for cells
that bound radioactive opiates
1. incubate membranes with radioactive opiate (opiate*).
2. wash out unbound opiate*
3. measure amount of bound opiate. Some will be bound to receptors,
some will just stick to membrane.
4. in second experiment. add opiate* and very large amount
of nonradioactive (cold) opiate.
5. cold opiate will displace opiate* at receptors but not at
nonspecific sites because there are such a large amount of nonspecific
sites.
6. number of receptors = binding of opiate* when no cold opiate
is added minus binding of opiate* when cold opiate is added. (I suggest
you try to diagram this for yourself).
C. there are many different types of opiate receptors:
mu is the type that binds morphine and is primarily responsible for pain
relief.
1. affinity for opiate is related to pain relief from that opiate.
2. mu receptor knockouts (KOs) are insensitive to morphine
3. naloxone binds to mu receptor.
D. naloxone, an opiate antagonist, is important in studying
mechanisms of pain treatment
a. If pain treatment uses opiate receptors, it is naloxone
reversible.
V. endogenous opiates:
A. many different ones, with different functions. enkephalins,
endorphins, dynorphins.
1. dynorphins also released by nerve cells
2. beta endorphins released by:
a. hypothalamic cells going to periaqueductal gray
and limbic system. A few processes of these hypothalamic cells go to spinal
cord
b. Pituitary, released into blood but function not
known.
B. made by cleaving large proteins
1. each protein can be cleaved in several ways to make
several different proteins.
2. All cells containing a particular protein do
not release same mix of cleavage products.
C. pain suppression not their only function, e.g. control
endocrine function.
D. are endogenous opiates addicting? (Wei Science 193:1262)
1. The experimenters infused control substance or endorphin
or enkephalin into central gray for 70 hours.
2. Then they gave the animals naloxone.
3. Animals had withdrawal symptoms if they had received
endorphin or enkephalin but not if they had received a control substance.
a. Withdrawal symptoms included shaking, try to
jump out of container.
4. When released by nerve cells endogenous are not addicting
because they are metabolized rapidly so the receptors are not flooded with
them for long periods of time. They are released only when they are needed.
VI. Why do we think they are involved in pain control?
A. enkephalins are released by nerve cells and bind to
opiate receptors.
B. Injection of enkephalins in periaqueductal gray
reduces pain.
C. Enkephalins are found in areas associated with perception
of pain and where morphine injection produces pain relief.
1. dorsal part of dorsal horn
2. periaqueductal gray
3. limbic system
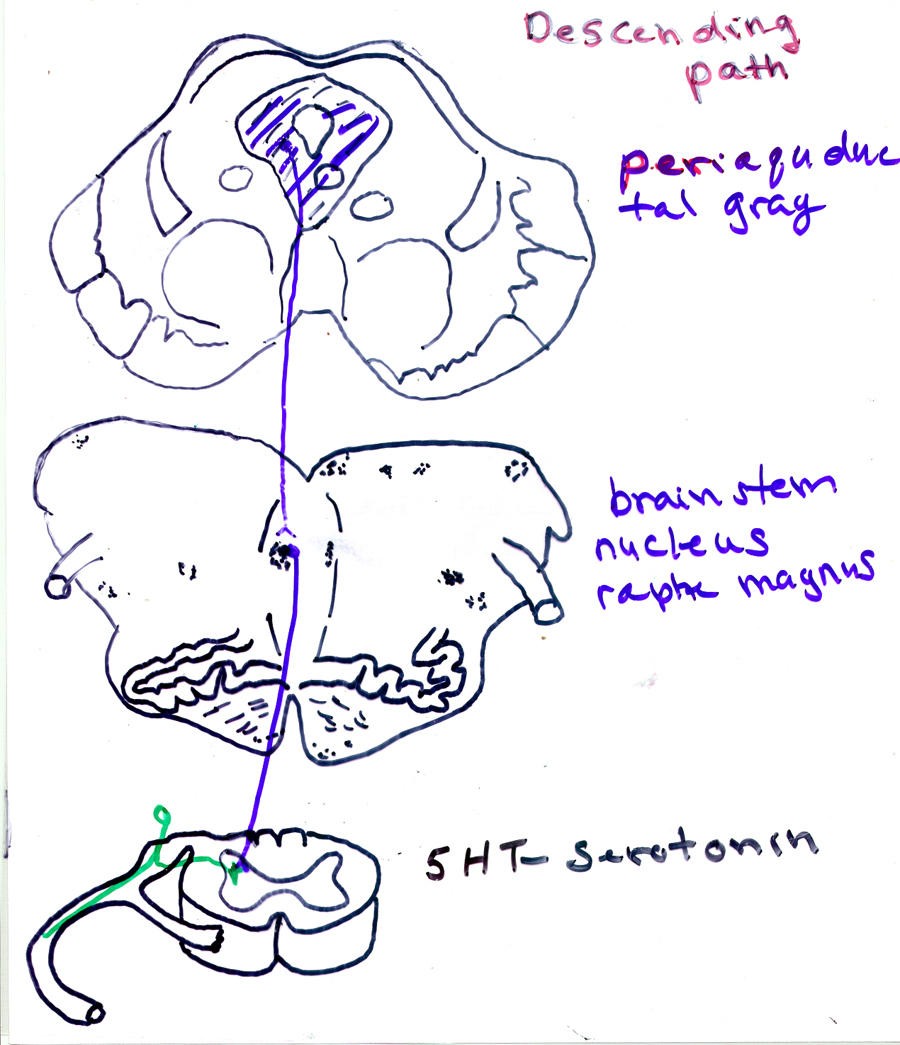
VII. How do descending signals modify transmission of pain information?
A. periaqueductal gray to raphe magnus to spinal cord.
B. opiates decrease duration of
AP in sensory terminal, release less transmitter.
1. Primary afferents have lots of opiate binding sites.
If you cut dorsal roots, opiate receptors in dorsal horn disappear
2. Morphine injected into spinal cord
can decrease release of glutamate and substance P
C. morphine hyperpolarizes dorsal horn neurons that respond to
noxious stimuli by activating a K+ conductance.
VIII. suppression of pain information by electrical stimulation:
stimulation produced analgesia (SPA).
A. Response to pain is reduced by stimulation of specific
brain regions. This is stimulation produced analgesia (SPA). SPA has some
resemblances to morphine analgesia.
1. decreases response to noxious stimuli, but not to touch
2. there is tolerance to effects of stimulation of central
gray.
3. pain relief can outlast stimulation by as much as 24
hrs.
B. Anatomy of SPA
1. stimulation is most effective in periaquductal gray
(PAG) or raphe magnus.
2. periaqueductal gray gets input from spinothalamic tract.
But this not for perception of pain rather for control of pain.
3. PAG sends inputs to nucleus raphe magnus in medulla
where it releases neurotensin
4. raphe sends information to spinal cord. raphe
neuron releases serotonin and perhaps also substance P onto spinal cord
interneurons that produce enkephalin.
5. These spinal cord interneurons may inhibit dorsal horn
cells or may prevent release of pain transmitter from primary afferent
terminal.
C. evidence that SPA works because opiate receptors are
stimulated.
1. sites where morphine works are sites where SPA works
2. SPA is naloxone reversible in both rats and humans
IX. Stress analgesia: need to reduce response to pain in time
of emergency.
A. This is a mechanism of pain suppression that uses
endogenous opiates and opiate receptors. It is similar to SPA except that
it uses natural stimuli rather than electrical stimulation of the brain.
B. Stress analgesia is partly naloxone reversible. Produced
by beta endorphin as well as enkephalin.
1. foot shock in rats causes tail flick. Tail flick latency
and endogenous opiates increase with repeated shocks. This is stress analgesia.
Stress analgesia can last min to hours.
a. may be an analogue of learned helplessness as occurs
primarily when shock is not avoidable
2. Humans: If stimulate nerve through skin, the threshold
for withdrawal decreases with repeated stimulation. This increase in threshold
is naloxone reversible.
3. Are stress and stimulation produced analgesia both due to
descending pathway that releases opiates in spinal cord?
a. breed animals for high and low stress analgesia with
swim test
b. high analgesia animals have much lower threshold for
SPA.
X. Other types of naturally occurring analgesia probably use
endogenous opiates and their receptors. Test is naloxone reversibility.
A. postoperative pain is probably reduced by opiate system; naloxone
increases it.
B. placebo analgesia is naloxone reversible under some
circumstances.
C. acupuncture analgesia naloxone reversible under some
conditions.
XI. Recent research on role of substance P and its receptors. How it
may lead to improved treatment of pain.
A. has a receptor called neurokinin-1 (NK-1).
B. knockout for this receptor
1. autoradiography using SP as the ligand shows no receptor
in brain or spinal cord.
C. normal mice increase response to increased mechanical
stimulation; knockouts to substance P receptor dont; that is,
knockouts have no intensity coding. Response was electromyographic response.
(KO may have higher firing rates due to decreased descending inhib).
D. Windup to repeated stimulation of C fibers only in WT not
in KO.
1. This suggests that Substance P is not involved in acute pain
but is involved in chronic pain.
E. behavioral responses to acute stimuli same in KO and WT.
F. swim analgesia is decreased in KOs.
G. KOs less aggressive
H. conclude that subP receptor needed for response to major pain
or invastion of territory. (data not all consistent with this interpretation)
XII. possible treatment for chronic pain: destroy cells with subP receptors.
Bind subP to a toxin. Inject into dorsal part of dorsal horn. Cells with
subP receptors internalize subP. But now they get toxin too and are killed.
Rats showed decreased pain responses
XIII. Pain: Is it all in your head? Answer: no. some of
it is in your spinal cord.